Nikhil Wagle, M.D., is using genomic analysis to better understand tumors and why some patients respond well to certain drugs, and other patients, who you’d think would also respond well, don’t respond at all or ultimately stop responding. Genomic analysis is the identification, measurement or comparison of genomic features, such as DNA sequence, structural variation, gene expression, or any regulatory or functional element that can be assessed at a genomic scale.
Dr. Wagle was recently named a Komen Scholar – an advisory group of distinguished leaders in breast cancer research, clinical practice, public health, advocacy and other relevant fields, who provide expertise and guidance to Susan G. Komen on research and other mission programs.
He spoke with Komen about what he’s learned about treatment response and how to improve outcomes for patients.
Q: How does analyzing tumors help you learn about a patient’s response to a breast cancer treatment?
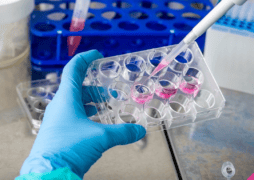
A: We collect tumor samples from patients so we can make sure we understand from those patients what their experience was, what drugs they got, what worked, what didn’t work. And then we look really closely at those tumors to try and understand the features of that particular individual’s tumor, and how we can relate those features to what happened to that patient.
If we do that over and over again in a lot of people, we start to see patterns. So, for example, on one hand everyone with one particular feature in their tumor may have responded really well to a particular drug. On the other hand, all the people with this other feature didn’t respond well to that drug. All of a sudden, we have something we can test, and maybe in future patients, say, “If you have this feature, you should get this drug. If you have this other feature, you shouldn’t get this drug.”
Q: What role does genomics play in that research?
A: Genomics is one of the features that we look at in the tumor samples. We collect tumor biopsies from patients and look at the DNA and the RNA and do a genomic analysis. Thanks to that analysis, we have found several reasons why tumors become resistant to some treatments. We’ve found several markers that have led us to new therapeutic strategies or new drugs. And we are starting to use that type of analysis to figure out what are better ways of treating breast cancer when it becomes resistant to therapies or even maybe upfront to prevent resistance from happening.
Q: Are you able to test a patient’s tumor periodically to see if it has become resistant?
A: Yes, when possible. We have learned in recent years that breast cancer evolves over time. If you look at breast cancer when it’s first diagnosed, it looks a particular way. Then someone gets treatment and let’s say the cancer recurs in the metastatic setting. That cancer looks a little different than the original cancer. Then let’s say they get some treatment in the metastatic setting, and then the tumor becomes resistant. That cancer looks a little different.
We know that the tumors keep acquiring new mutations or new features that cause them to either be more metastatic, more aggressive, or more resistant to treatment. We have these incredible patients who volunteer to participate in our work and many of them are willing to share not just one sample, but multiple samples– or come back and get another blood sample or give another biopsy, so that we can track these things over time and look at tumor evolution.
Q: How does what you’re learning about which patients respond to a specific therapy and which ones don’t, inform your lab research?
A: When we say, “Patients whose tumors look like this tend to respond well to this drug, but patients whose tumors look like this tend to not,” it is a hypothesis and not a definite answer.
So, then we have to prove it to ourselves. In my laboratory, we’ll take a mutation, for example, and then we make it in the model system, and we test it. We’ll use a drug and see if the mutation we’re testing causes resistance to the drug. And if it does, then we feel like we’re onto something. Then we try and overcome that resistance. If we can come up with a strategy that reverses the resistance, then we get excited about maybe taking that to a clinical trial.
Q: There’s another thing you’re passionate about, called “Count Me In.” Tell us about this program and how people can get involved.
A: We’ve used social media, the Internet, advocacy groups and other ways to ask people to participate in research wherever they live, so that any researcher who wants to use the data, can. My hope is that having all this data will really accelerate science, accelerate discoveries and do it in a cost-effective way.
Q: What has been the patient response to “Count Me In”?
A: We launched the Metastatic Breast Cancer Project in 2015, and over the last six years more than 6,000 women and men with metastatic breast cancer, which is a very large number of patients to participate in a single study like this, have signed up.
It is an opportunity for patients to take some control and have some say in what’s happening in a time where often they don’t have a lot of control. Our experience with patients who are participating in this type of research is they want to help. And there’s also this incredible recognition that patients know that this research may not be able to help them and yet they want to participate because it might help the next person. Learn more about “Count Me In” at https://joincountmein.org/
*Dr. Wagle is an Assistant Professor of Medicine at Harvard Medical School, a medical oncologist at Dana-Farber Cancer Institute and an Institute Member at the Broad Institute of MIT and Harvard.